
Fibromyalgia is a leading cause of chronic pain affecting millions of Americans every day. Researchers hypothesize that central sensitization is the primary mechanism involved, but there are many other factors including genetics, immunological, psychological, and hormones that influence the development of fibromyalgia. Central sentization refers to a process called “wind-up” where the central nervous system gets regulated into a persistent state of high reactivity. This persistent or wound up state of reactivity lowers the threshold for what causes pain and can create extreme pain even with minimal stimulus. This phenomena is believed to be related to neuroplasticity which is mediated by the N-Methyl-D-aspartate (NMDA) receptors located in the spinal cord.
So how exactly do ketamine infusions help in fibromyalgia?
Ketamine’s most immediate mechanism of action is to block NMDA receptors. It is the most potent clinically available NMDA receptor antagonist today. By blocking the activity of the NMDA receptor, ketamine seems to reset the altered pain receptors that have become hypersensitized in patients with fibromyalgia.
Over the long term, ketamine has been shown to alter the expression of NMDA receptors and reduce neuro-inflammation in the rat and mouse models of pain, which has been correlated with reductions in neuropathic pain. Additionally, ketamine increases brain-derived neurotrophic factor (BDNF) resulting in neurogenesis and synaptic changes to the central nervous system - both of which are key to neuroplasticity.
Furthermore, ketamine has also been shown to inhibit activity of the default mode network (DMN) in the brain, portions of the brain that are active when the mind is believed to be at rest, i.e. daydreaming and mind-wandering. Interestingly, hyperconnectivity of the DMN has been linked to rumination in depression and chronic pain, like fibromyalgia.
The “off-label” use of ketamine for a variety of conditions, such as depression, anxiety, PTSD, and chronic pain is becoming more common. For example, the number of ketamine infusions centers in the United States has increased allowing more patients therapeutic opportunities. National organizations, such as the American Society of Ketamine Physicians and Kriya Institute, have formed to increase awareness of ketamine by bringing physicians, psychologists, and nurses together. Additionally, ketamine is being used in the emergency department as an alternative to morphine for pain control and some paramedics are even administering ketamine in ambulances. Most recently, the U.S. Food & Drug Administration (FDA) has approved of intranasal esketamine *blog link* for treatment-resistant depression, which lends support to the safety & efficacy of long-term ketamine for maintenance of symptoms beyond the initial series of infusions.
Fibromyalgia: Prevalence, Symptoms, and Diagnosis
Fibromyalgia affects an estimated 10 million Americans and an estimated 3-6% of people worldwide. It is much more common in women affecting up to 75 - 90%, but it also affects men and children of all ethnic groups. This disorder is often seen in families, among siblings, and children of women affected by it. Fibromyalgia seems more common as age advances, so that by 80 years of age approximately 8% of people meet the American College of Rheumatology classification criteria.
Fibromyalgia is diagnosed based upon patient reports and on clinical assessment. Unfortunately, there is no specific laboratory test or reliable biomarker for the diagnosis of fibromyalgia. The 2010/2011 American College of Rheumatology (ACR) criteria with the 2016 revision included the “generalized pain criteria,” defined as the presence of pain in 4 out of the 5 possible body regions, but there is still uncertainty and lack of accuracy in clinical practice.
“Fibromyalgia may now be diagnosed in adults when all of the following criteria are met:
1. Generalized pain, defined as pain in at least 4 of 5 regions, is present.
2. Symptoms have been present at a similar level for at least 3 months.
3. Widespread pain index (WPI) ≥ 7 and symptom severity scale (SSS) score ≥ 5 OR WPI of 4–6 and SSS score ≥ 9.
4. A diagnosis of fibromyalgia is valid irrespective of other diagnoses. A diagnosis of fibromyalgia does not exclude the presence of other clinically important illnesses.”
In 2018, a group of clinicians and basic scientists came together and created the ACTION-APS Pain Taxonomy (AAPT) initiative to develop a diagnostic system that would be more clinically relevant and consistent for chronic pain disorders.
The AAPT Taxonomy considers 5 dimensions in diagnosing fibromyalgia:
Dimension 1 - Core Diagnostic Criteria:
Presence of multisite pain, defined as the presence of pain in 6 out of 9 possible sites together with moderate to severe fatigue or sleep problems assessed by a healthcare professional
Symptoms present for at least 3 months
Dimension 2 - Common Features:
Tenderness to touch (positive tender points exam)
Dyscognition (e.g. trouble concentrating, forgetfulness, disorganized, or slow thinking
Musculoskeletal stiffness and environmental sensitivity (e.g. bright lights, loud noises, strong scents, and cold)
Dimension 3 - Common medical comorbidities:
Somatic pain disorders
Psychiatric conditions
Sleep disorders
Somatic diseases
Dimension 4 - Neurobiological, psychological, and functions consequences:
Poor quality of life
High costs that indirectly stem from the burden of fibromyalgia
Dimension 5 - Putative neurobiological and psychosocial mechanisms, risk factors, and protective factors:
Familitary for functional pain disorders
Environmental stressors that may trigger fibromyalgia:
Early lifetime adverse events
Trauma
Medical conditions
Psychosocial stressors
Central sensitization - A Deeper Level
Central sensitization can be defined as “a state in which the central nervous system amplifies sensory input” and creates an enhanced response to sensation (AKA “wind-up”). Changes at the neuronal level increases sensitivity for future stimulation. On the cellular level, central sensitization alters the neurons that sense pain via increases in membrane excitability, stronger synaptic strength, and the diminished ability to inhibit transmission of sensation. Heightened sensitivity can result in the perception of pain from non-painful stimuli (allodynia) and greater pain than would be expected from painful stimuli (hyperalgesia). This “wind-up” state is believed to be related to neuroplasticity which is mediated by the N-Methyl-D-aspartate (NMDA) receptors located in the postsynaptic membrane in the dorsal horn of the spinal cord.
What also modulates the NMDA receptor? Ketamine.

Ketamine blocks the NMDA receptors found in the dorsal horn of the spinal cord, which seems to “reset” the pain receptors. Illustration by Kimberly Ko, MD. © 2019.
A double-blind and placebo-controlled trial took 31 patients with fibromyalgia and gave a 9 morphine, 11 lidocaine, and 11 patients ketamine. This study looked at the patient’s pain tolerance at tender points as well as pain intensity, pressure pain threshold, muscle strength, and static muscle endurance. The study found that morphine did not result in significant change, and lidocaine showed decreased pain during and after the infusion. What was interesting was that the ketamine infusion showed a significant pain reduction during and after, which supports the hypothesis that NMDA receptors are very much part of the pain mechanisms in fibromyalgia.
One of the ways ketamine is able to reset these altered pain receptors is by blocking the activity of the NMDA receptor. While it is not immediately clear how exactly this NMDA receptor blockage helps, the thought is the disruption of this cycle of hypersensitivity helps with re-modulating the nervous system to a more balanced state, or “resetting” the pain receptors. We believe, however, there are many more ways that ketamine is able to help reduce the symptoms of fibromyalgia.
Small Fiber Neuropathy and Neuro-Inflammation in Fibromyalgia
There is also support that small fiber neuropathy (SFN) plays a role in fibromyalgia. Although SFN is a separate diagnosis, researchers found that the prevalence of small fiber neuropathy was 49% in patients suffering from fibromyalgia. Small fiber neuropathy occurs when damage to the peripheral nerves affects the small myelinated fibers or unmyelinated C fibers, resulting in loss of fibers or abnormal fiber shapes. Unfortunately, the cause of small fiber abnormalities is not well understood, but it may be related to a pro-inflammatory state at the level of the nerve fibers.
Inflammation is a normal process of the body. It is the body’s immune system at work to prevent infections from viruses, bacteria, and fungi. The immune system has a miraculous ability to detect and destroy foreign invaders that attempt to establish a foothold in your body. However, there are times when the immune system starts attacking the cells it was designed to protect.
One of the key components of inflammation is tumor necrosis factor alpha (also known as TNF-α). TNF-α is important in cell signaling for the immune system. Ketamine is a potent anti-inflammatory agent and has been shown to reduce TNF-α levels in humans, horses, and rat models. Furthermore, ketamine has been shown to reduce other neuropathy related inflammatory markers as well.
Furthermore, neuroimmune activation is one of the possible mechanisms that may be involved in the central nervous system dysfunction described in fibromyalgia. Recently, a combined research group from Sweden and the United States demonstrated for the first time the presence of activated glia, resulting in active neuro-inflammation in the brains of fibromyalgia patients. This could mean ketamine’s effect on fibromyalgia may not only be related to NMDA receptor blockade, but also it’s anti-inflammatory action in the peripheral nerves and inside of the central nervous system.
Ketamine’s Role in Neuroplasticity

Multipolar Neuron. Wikimedia Commons.
The other key area ketamine plays a role is in neuroplasticity. Chronic pain actually reshapes and alters the brain. Preclinical data suggests that chronic pain may cause significant changes in hippocampal plasticity, including a reduction of new neurons in the hippocampus (a portion of the brain related to learning, memory, mood regulation, and stress response.) It has previously been believed that a person is born with a finite number of neurons which will deteriorate over time. However, recent scientific data shows that neurons are continually being generated in adult brains (i.e. amygdala, hypothalamus, and hippocampus).
Ketamine is known to increase brain derived neurotrophic factor (BDNF). BDNF regulates many of the processes within neurogenesis, such as differentiation and survival. Furthermore, higher levels of BDNF have been involved in long-term potentiation of neurons and synaptic plasticity. This may explain why higher levels of BDNF are associated with enhanced memory and may also reduce the effects of chronic stress, fibromyalgia, and cognitive decline.
Depression and Anxiety Linked to Fibromyalgia
Depression and anxiety are commonly seen with fibromyalgia and have inter-related symptoms. This makes sense because being in a state of constant, diffuse pain will absolutely affect every part of your life. Depression and anxiety can even be painful to the mind. One theory of chronic pain, from psychologist Dr. Ronald Melzack, involves the complex physiological and psychological interplay resulting in a multidimensional experience. This neuromatrix model explains that it’s not only the central nervous system and nerves, but also includes neurotransmitters, hormones, and receptors. Pain is believed to be produced by the output of a widely distributed neural network rather than directly by sensory input only.
Could it be possible that fibromyalgia, depression, and anxiety actually all have the same root cause that is still yet to be fully understood by scientists?
One clinical point of data may lend support to this idea. Sometimes antidepressants are prescribed for fibromyalgia as part of the treatment regimen. For example, duloxetine was originally developed as a drug for depression and anxiety. Duloxetine is a selective serotonin and norepinephrine reuptake inhibitor (SNRI), but the FDA approved it for the treatment of fibromyalgia because of research-backed clinical evidence supporting its use for this condition.
This is where the bio-psycho-social-spiritual model of medicine comes into play. It’s important to consider other factors beyond biology. Something to consider is that there really is no separation of mind, body, and spirit. One analogy of this is a map. For example, if you look at the border between California and Arizona on the map there is a thick black-lined border. But if you actually go to the physical location at the state line between California and Arizona, there is no border.
Similarly, there is no border between mind, body, and spirit. Every disease has a psychological, sociological, and a spiritual component to it. Accordingly, we ask our patients, "How’s your exercise? How’s your meditation? How’s your sleep? How are your relationships going? How is your diet? What are you feeding your body and your mind?”
We highly encourage having strong relationships with your therapist, psychologist, psychiatrist, spiritual counselor, life coach, health coach, spiritual & local community. Furthermore, we suggest daily physical exercise, meditation, adequate sleep, journaling, listening to uplifting music, eating a healthy diet, associating with positive friends, & gratitude exercises.
Ketamine Affects the Default Mode Network (DMN)
The default mode network (sometimes called simply the default network or the DMN) refers to an interconnected group of brain structures that are hypothesized to be part of a functional system. The DMN includes areas of the brain, which researchers found to have higher activity when the mind was supposed to be at rest. For example, the DMN is active when you are daydreaming, thinking about the future, replaying memories, etc. without a specific goal in mind. Now, why would we care about this?
One study looked at 16 patients with fibromyalgia and compared them to 15 control subjects without fibromyalgia using MRI scans of the brain. They found there was altered functional connectivity between DMN regions and a variety of areas related pain, cognitive and emotional processing in patients with fibromyalgia. Altered DMN activity and functional connectivity is also found in depression as well.
In both of these disorders, there is much rumination. Rumination is where you have repetitive thoughts. Those who deal with fibromyalgia may replay moments of suffering or sadness over and over in their mind. This prevents them from healing and creating room for more positive emotions and memories. Additionally, those with pain may become fixated on the pain itself, or replay the events which lead to them having the pain. This type of circular, overactive thinking occurs in the DMN. Reducing activity in the DMN can decrease rumination, which in turn can reduce pain and depressed feelings.
Here’s the interesting part - ketamine actually reduces the functional activity in the DMN! One study showed that the connectivity of the DMN along with another portion of the brain, the dorsal nexus, was decreased after ketamine infusions. So ketamine can effectively turn down the overactive areas in our mind, which can support improved mood and less pain.

Magnetic resonance imaging of areas of the brain in the default mode network. Public Domain from Wikipedia.
A Case Report of A Patient with Fibromyalgia from Reset Ketamine
Megan* knew something was wrong. In her twenties, she had popping pains throughout her body, pains she largely ignored. But as she got older, the discomfort became more insistent. Some days, her energy level was so low she couldn’t get off the couch. Other times, her vision blurred so much that she dared not drive. “I found myself staying home more and more. My life was slipping away from me.”
As Megan’s world got smaller, her depression and body pains grew larger. She went to her primary medical doctor who referred her to a rheumatologist, a doctor who specializes in the treatment of musculoskeletal system and systemic auto-immune diseases. The rheumatologist performed a series of blood tests and could not find any major abnormalities to explain Megan’s pain. Ultimately, she was diagnosed with fibromyalgia and started on various pain medications and antidepressants.
Although it’s hard to diagnose, people with fibromyalgia commonly report fatigue, depression and a wide range of physical pain. These symptoms can lead patients to feel isolated and homebound, a condition which exacerbates the problems of illness. Some people find that depression can make it hard to address underlying issues.
Megan tried the medications but found the side effects intolerable and felt quite hopeless. She turned to massage therapy, psychotherapy, and CBD products, but only found partial relief. Serendipitously, she found out that Reset Ketamine was opening in the Palm Springs, California and requested a consultation for ketamine infusions.
Prior to the first infusion, Megan’s Fibromyalgia Impact Questionnaire (FIQ) score was initially rated at 64 and after the initial series of infusions her score went down to 15.
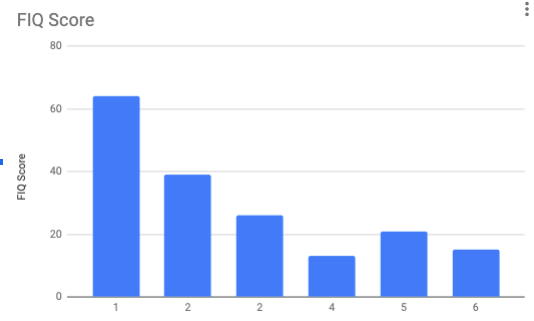
Fibromyalgia Impact Questionnaire (FIQ) Score - Reset Ketamine Patient
She received several boosters over the next few months and her last FIQ score was 5.
The ketamine infusions were a catalyst for Megan to create lifestyle changes that created a positive upward spiral in her life. Megan changed her diet, started working out and meditating daily, ended an unhealthy relationship, and started a new job that better aligned with her life purpose.
*Name and Identifying Details Changed
“Now, I continue to manage my condition with diet and the practices of meditation and other factors I learned from Dr. Ko. I am a vastly different and 100% more functional person than I was the day I walked in and met Dr. Ko. He doesn’t just practice medicine, he approaches each patient on a holistic level as well, taking the WHOLE of you into consideration - mind, body and spirit for a complete and most efficient and lasting healing.
I had very little to zero side effects and Dr. Ko is right there to literally hold your hand during treatment (something he has done for me many times) if need be. He is caring, kind, passionate and down right miraculous. Don’t be afraid to have an open mind and take the plunge to start your healing. You are not in just good hands, but the best hands with Dr. Ko.
I am eternally grateful to this man for giving me my life and the quality of my life back when I was deep in despair at a young age thinking I would have to live that way forever.
I referred a friend after my treatment who was also suffering greatly, and he too is doing phenomenal after years of suffering and sickness. My hope is that many people will be reached, read this and receive relief for themselves as well.”
Ketamine Can Also Help Reduce Neuropathic Pain
Ketamine infusions have been extensively used to treat unmanageable neuropathic pain conditions. The infusion protocol varies greatly depending on the administerer. Because of this variation, it is difficult to compare one protocol to another and to determine what exactly the best protocol is. Careful examination of the published literature does suggest that ketamine is useful in treating neuropathic pain conditions, for example, trigeminal neuralgia, post-herpetic neuralgia, complex regional pain syndrome, and fibromyalgia.
A systematic review of the published literature on ketamine and neuropathic pain suggest three major commonalities:
Longer durations of infusions provide longer lasting pain relief. Studies with infusions lasting one hour or less reported a decrease in the degree of pain relief. Longer infusions provided over the course of several days may provide longer lasting benefits opposed to a single infusion or shorter duration infusions.
The higher the total dose of ketamine administered the higher the degree of pain relief and possibly, the longer the duration of relief. The rate of infusion does not appear to affect the degree or duration of pain relief.
Almost all patients, regardless of protocol, experience side effects such as nausea, headaches and tiredness. Coadministration of medications like ondansetron reduced side effects.
Overall, higher total ketamine doses, longer infusion durations, and coadministration of supplementary drugs are associated with increased duration of neuropathic pain relief. Because there is not a standardized method for treating complex regional pain syndrome (CRPS), postherpetic neuralgia, fibromyalgia using ketamine infusions, further research will need to be conducted on what is the optimal protocol for treating neuropathic pain.
Reset Ketamine’s Protocol for Fibromyalgia
As you know already, there is no standard ketamine infusion guideline for fibromyalgia, so we have created our own protocol based upon clinical experience, patient comfort, and basic science research.
First, there are four stages of ketamine infusions at Reset Ketamine: 1) Preparation, 2) Intention, 3) Experience, 4) Integration. We are consciously proactive about creating the ideal mindset prior to the infusion and an optimal environment for patients at the clinic (AKA “set and setting).
For the timing and frequency, we recommend 6 infusions for the initiation series over a 2-3 week time period. We believe it’s important to give a 1-3 days between infusions to let the brain rest and allow time for changes at the neuronal level.
Each infusion is 85 minutes in duration, but the patient is in the clinic for about 2.5 hours from beginning to end. The first dose of ketamine typically begins at 1 mg/kg. We gradually increase the dose of ketamine with each successive infusion, based upon the vital signs during infusion and patient effect level.
We provide an eye mask and headphones with a specific playlist since research shows that music has a significant effect on patients during ketamine treatments.
Sometimes, we administer intravenous magnesium, ondansetron (aka Zofran), and/or a anti-hypertensive medication (i.e. Labetalol), depending upon the patients symptoms and vital signs.
Generally, we avoid the use of benzodiazepines (like Ativan or Versed) as this can reduce the psychotropic effect of ketamine. We believe the experiential effect of ketamine plays a crucial role in healing.
We also recommend having an appointment scheduled with your psychotherapist or counselor after each infusion to help make meaning from the experience. We believe it’s best to use ketamine as a catalyst to help get you “unstuck.”
After the initial series of 6 infusions, some of our patients will need boosters infusions. The timing of the boosters are dependent upon the severity of the symptoms.
Related Questions
Why isn’t my doctor recommending ketamine infusions?
The medical profession is slow to change, and even slower to adopt new practices and new medicines. Believe it or not, at one point in history, doctors did not believe in handwashing. (Read our post on “Ketamine’s Slow Acceptance By the Medical Community”) But not only does the medical profession have to convince approving bodies that a medication or treatment is safe, they then have to get buy-in from other medical professionals themselves.
So why aren’t more doctors and mental health care providers shouting from rooftops wanting to share this amazing medication with you? Here are three reasons why:
1. They simply don’t know about ketamine: When a future doctor goes to medical school they learn a ton of information. They learn about ketamine as an anesthetic agent, not as a treatment for mood disorders. In residency (where a doctor gains specialty training) there are only a handful of specialities, namely emergency medicine, critical care, and anesthesia, who regularly administer ketamine and let alone are comfortable in using it. Also, if your doctor or mental health professional is not following the latest and innovative treatments they may not know the growing role of ketamine to treat your condition.
2. They simply don’t believe in ketamine or are biased: Doctors are humans, humans are creatures of habit. They may not believe in using unconventional treatments, or don’t agree with using traditionally accepted medications in novel ways. Your doctor may have a religious or moral bias against medications that are dubbed “psychedelics”, as ketamine can cause psychedelic experiences at certain doses.
3. They don’t know how to advise you on the use of ketamine: Maybe your doctor has seen that same video online, read the latest medical journal articles about ketamine, and even wants to encourage you to give it a try! Well, they may not advise you to try ketamine because they don’t know how or where to send you. Maybe they know of a doctor who would be great for you, but lives on the other side of the country. Maybe there is no one they know in your local medical community they could refer you to. Or because they don’t have experience with it they don’t want you to get mistreated or hurt...so they simply don’t recommend it.
So the next time you see your doctor or mental healthcare provider, and think about discussing ketamine with them, keep these reasons in mind. Perhaps these reasons will give you a little perspective from where your doctor is coming from when you hear their responses.
What are the long-term consequences of ketamine infusions?
Bladder Damage - There have been reports of ketamine-induced cystitis in heavy users of ketamine. The symptoms of this are frequency, urgency, painful urination, and bladder pain. Essentially, this feels like a urinary tract infection but without a bacterial cause. Ketamine-induced cystitis is believed to be caused by ulceration to the bladder lining and chronic inflammation, but the exact mechanism is unclear. This has been noted in particular when people are abusing it recreationally, frequently, and in unsupervised settings. However, it is very possible that ketamine treatments may cause bladder irritation.
It is important to be aware of this and let your doctor know immediately if you experience any difficulties with urination. You may need a referral to a urologist if this occurs for urological treatment. Fortunately, ketamine-induced cystitis can resolve once ketamine infusions are completely stopped.
Liver Damage. Liver injury was also found in about 10% of chronic abusers of ketamine. This happened in the setting of chronic, high dose, frequent, unmonitored self-administered ketamine. However, there are also reports of ketamine-induced liver injury in the clinical setting. One article reports three patients who developed hepatotoxicity when they received continuous 100 hour infusions separated by 16 days for the treatment of complex regional pain syndrome (CRPS). Fortunately, their lab results showed normal liver function tests at two month follow-up.
Will I become addicted to ketamine?
This is a common question from some patients, so we actually devoted a whole blog post on this topic here: Are Ketamine Infusions Addictive?
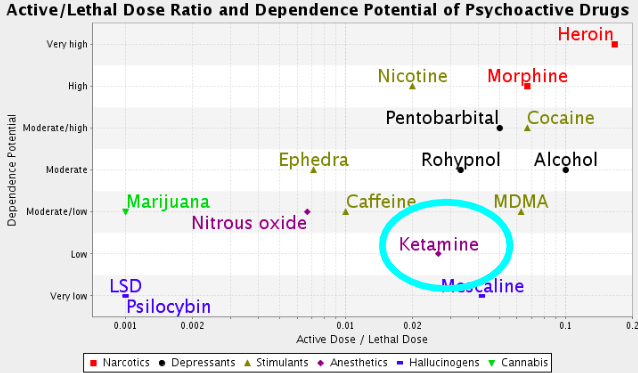
The diagram shows the dependence potential and the relation between active and lethal dose of some psychoactive substances. Wikipedia.
This chart above shows that ketamine has a low potential for abuse, much lower than alcohol, opioids, coffee, or tobacco. So, ketamine definitely has a small potential for abuse, but the bottom line is that addiction is highly unlikely in the set and setting of a professionally monitored infusions.

Fibromyalgia is a leading cause of chronic pain affecting millions of Americans every day. Researchers hypothesize that central sensitization is the primary mechanism involved, but there are many other factors including genetics, immunological, psychological, and hormones that influence the development of fibromyalgia. Central sentization refers to a process called “wind-up” where the central nervous system gets regulated into a persistent state of high reactivity. This persistent or wound up state of reactivity lowers the threshold for what causes pain and can create extreme pain even with minimal stimulus. This phenomena is believed to be related to neuroplasticity which is mediated by the N-Methyl-D-aspartate (NMDA) receptors located in the spinal cord.
So how exactly do ketamine infusions help in fibromyalgia?
Ketamine’s most immediate mechanism of action is to block NMDA receptors. It is the most potent clinically available NMDA receptor antagonist today. By blocking the activity of the NMDA receptor, ketamine seems to reset the altered pain receptors that have become hypersensitized in patients with fibromyalgia.
CONTACT RESET KETAMINE
IF YOU OR SOMEONE YOU LOVE IS SUFFERING FROM FIBROMYALGIA, ANXIETY, PTSD, DEPRESSION, OCD, MIGRAINES, FIBROMYALGIA, OR CHRONIC PAIN, PLEASE CONTACT US NOW FOR A CONSULTATION TO SEE IF YOU WOULD BE AN IDEAL CANDIDATE FOR KETAMINE INFUSIONS.
SERVING PALM SPRINGS, PALM DESERT, RANCHO MIRAGE, CATHEDRAL CITY, JOSHUA TREE, 29 PALMS, IDYLLWILD, REDLANDS, LOMA LINDA, BEAUMONT, BANNING, ONTARIO, RIVERSIDE, LOS ANGELES, ORANGE COUNTY, SAN DIEGO, HOLLYWOOD, LONG BEACH, SANTA MONICA, AND ALL OF CALIFORNIA.
References
“2010 Fibromyalgia Diagnostic Criteria - Excerpt.” American College of Rheumatology, 2010, www.rheumatology.org/
Arnold, Lesley M., et al., “AAPT Diagnostic Criteria for Fibromyalgia.” The Journal of Pain, 2018, doi:10.1016/j.jpain.2018.10.008.
Atzeni, F, et al., “ One year in review 2019: fibromyalgia.” Clinical and Experimental Rheumatology Online, 2019 Jan-Feb;37 Suppl 116(1):3-10. Epub 2019 Feb 6.
Bellato E, Marini E, Castoldi F, et al., Fibromyalgia syndrome: etiology, pathogenesis, diagnosis, and treatment [published correction appears in Pain Res Treat. 2013;2013:960270]. Pain Res Treat. 2012;2012:426130. doi:10.1155/2012/426130
Dahan, Albert, et al., “Targeting the Innate Repair Receptor to Treat Neuropathy.” PAIN Reports, vol. 1, no. 1, 2016, doi:10.1097/pr9.0000000000000566.
Fallon, Nicholas, et al., “Functional Connectivity with the Default Mode Network Is Altered in Fibromyalgia Patients.” Plos One, vol. 11, no. 7, 2016, doi:10.1371/journal.pone.0159198.
Fleming, Kevin C., and Mary M. Volcheck. “Central Sensitization Syndrome and the Initial Evaluation of a Patient with Fibromyalgia: A Review.” Rambam Maimonides Medical Journal, vol. 6, no. 2, 2015, doi:10.5041/rmmj.10204.
Graven-Nielsen, Thomas, et al., “Ketamine Reduces Muscle Pain, Temporal Summation, and Referred Pain in Fibromyalgia Patients.” Pain, vol. 85, no. 3, 2000, pp. 483–491., doi:10.1016/s0304-3959(99)00308-5.
Littlejohn, Geoffrey, and Emma Guymer. “Modulation of NMDA Receptor Activity in Fibromyalgia.” Biomedicines, vol. 5, no. 4, 2017, p. 15., doi:10.3390/biomedicines5020015.
Loix S, De Kock M, Henin P. “The anti-inflammatory effects of ketamine: state of the art”. Acta Anaesthesiol Belg. 2011;62(1):47–58.
Maher, D. P., Chen, L., & Mao, J. (2017). Intravenous Ketamine Infusions for Neuropathic Pain Management. Anesthesia & Analgesia, 124(2), 661-674. doi:10.1213/ane.0000000000001787
McAllister, Murray J. “What Is Central Sensitization?” Institute for Chronic Pain, 23 Mar. 2013, www.instituteforchronicpain.org/understanding-chronic-pain/what-is-chronic-pain/central-sensitization.
Melzack, R. “Pain and the neuromatrix in the brain.” Journal of Dental Education. Dec 2001, 65 (12) 1378-1382.
Noppers IM, et al. “Drug-Induced Liver Injury Following a Repeated Course of Ketamine Treatment for Chronic Pain in CRPS Type 1 Patients: A Report of 3 Cases.” 2011 Sep;152(9):2173-8. doi: 10.1016/j.pain.2011.03.026.
“Prevalence.” National Fibromyalgia Association (NFA), www.fmaware.org/about-fibromyalgia/prevalence/.
Sörensen, J., et al.,“Pain Analysis in Patients with Fibromyalgia:Effects of Intravenous Morphine, Lidocaine, and Ketamine.” Scandinavian Journal of Rheumatology, vol. 24, no. 6, 1995, pp. 360–365., doi:10.3109/03009749509095181.
Tsai, Yao Chou, and Hann-Chorng Kuo. “Ketamine Cystitis: Its Urological Impact and Management.” Urological Science, vol. 26, no. 3, 2015, pp. 153–157., doi:10.1016/j.urols.2014.11.003.
Wolfe, Frederick, et al., “The American College of Rheumatology Preliminary Diagnostic Criteria for Fibromyalgia and Measurement of Symptom Severity.” Arthritis Care & Research, vol. 62, no. 5, 2010, pp. 600–610., doi:10.1002/acr.20140.
Wolfe, Frederick, et al., “2016 Revisions to the 2010/2011 Fibromyalgia Diagnostic Criteria.” Seminars in Arthritis and Rheumatism, vol. 46, no. 3, 2016, pp. 319–329., doi:10.1016/j.semarthrit.2016.08.012.
Wong, G. L., Tam, Y., Ng, C., Chan, A. W., Choi, P. C., Chu, W. C., . . . Wong, V. W. (2014). Liver Injury Is Common Among Chronic Abusers of Ketamine. Clinical Gastroenterology and Hepatology,12(10). doi:10.1016/j.cgh.2014.01.041
Wright CL, Mist SD, Ross RL, Jones KD. Duloxetine for the treatment of fibromyalgia. Expert Rev Clin Immunol. 2010;6(5):745–756. doi:10.1586/eci.10.6
You Might Also Like:









In this blog, we share ketamine’s mechanism in treating chronic pain and why it’s more effective in treating some types of pain more than others. We also talk about the things you have to consider when treating pain with ketamine and why ketamine isn’t the only “magic potion” you need to fully heal.